 When Jeanette asked me to write an article for Lightwaves, I debated about the subject. I decided on this title since this is where we all live 24/7: the oral cavity. I wanted to make sure that my ALD Buddies didn’t start to slack off on their COVID-19 protocols, even though we have access to vaccines and many are relaxing their mask mandates. Nine people that I know that have been triple vaccinated have come down with the virus and one very seriously.
When Jeanette asked me to write an article for Lightwaves, I debated about the subject. I decided on this title since this is where we all live 24/7: the oral cavity. I wanted to make sure that my ALD Buddies didn’t start to slack off on their COVID-19 protocols, even though we have access to vaccines and many are relaxing their mask mandates. Nine people that I know that have been triple vaccinated have come down with the virus and one very seriously.
We have all been living and dealing with COVID-19 for two years and as this pandemic has been part of our daily living for this period, the research has expanded tremendously. Our population has been dealing with different forms of the corona virus since the early 1900s. Corona viruses produce the common cold, severe acute respiratory syndrome (SARS), Middle East respiratory syndrome (MERS), novel coronavirus, SARS-CoV-2, and now “COVID-19.” Cytokine storms were responsible for the 50 million deaths during the 1918 influenza pandemic and many deaths during the SARS “the bird flu H5N1”epidemic in 2003. I lost 5 uncles to the Spanish Flu and 8 members of my family were infected by CVOID-19. All in healthcare living in New York.
So how does this virus cause such havoc and death? The usual response is that the immune system attacks the virus causing inflammation and fever. However, in severe cases, the immune system goes wild, and causes excessive inflammatory cytokine production and immune hyperactivity. This exaggerated immune response is called “the Cytokine Storm”. It leads to Acute Respiratory Distress Syndrome or “ARDS” which leads to fever, multi0organ failure, and death.
It was originally thought that the virus lived and reproduced in the nasal passages and lungs and that it showed up in the oral cavity if we shallowed some nasal discharge or coughed up some phlegm from our lungs. However, recent research has found that this virus lives and replicates in the oral cavity. The best publication on this is, “SARS-CoV-2, infection of the oral cavity and saliva” published in Nature Magazine Published: 25 March 2021 27, pages892–903 (2021), Ni Huang, Paola Pérez, Kevin M. Byrd. “Mouth may transmit virus to lungs, digestive system” National Institutes of Health and University of North Carolina at Chapel Hill
They had several questions that they wanted answered;
- Is the infection in the oral cavity and saliva? They analyzed two single-cell RNA sequencing datasets of the salivary glands and gingiva and found: Saliva from COVID-infected individuals harbored epithelial cells exhibiting ACE2 and TMPRSS expression and sustained COVID infection. This confirmed COVID infection in the glands and mucosa.
- Is the mouth a route of infection and incubator for the virus? This is why individuals have altered/loss of taste and dry mouth. The virus could potentially come from nasal drainage or phlegm coughed up from the lungs, but this doesn’t explain how the virus gets into the saliva of people who are asymptomatic.
- Could some of the virus in saliva be coming from infected tissues in the mouth? They surveyed oral tissues and found some cells in the salivary glands, gingival cells and tissues lining the oral cavity contained RNA for two key "entry proteins" — the ACE2 receptor and the TMPRSS2 enzyme. The virus needs both entry proteins to gain access to cells. This allowed entry, making them susceptible to infection.
- Is saliva a route for COVID-19 transmission? COVID-19 RNA was present in more than half of the salivary glands collected from patients who had died. Cells that shed from the mouth into saliva contained RNA for COVID-19 and the entry proteins. They found specific sequences of viral RNA that indicated cells were actively making new copies of the virus. Even in asymptomatic or mild cases
- Are infected oral tissues a source of the virus in saliva? They took saliva from eight asymptomatic patients and mixed with healthy cells grown in a petri dish. The saliva from two of the patients caused the healthy cells to become infected. Therefore, it is possible for asymptomatic people to transmit the virus to others through saliva. The virus was present in the saliva of those who had changes to their taste/smell.
- Is the oral infection the reason for oral symptoms? Patients with mild or asymptomatic COVID-19 were more likely to report a loss of taste and smell if they had virus in their saliva, "When infected saliva is swallowed or tiny particles of it are inhaled, we think it can potentially transmit COVID further into our throats, our lungs or even our guts," Dr. Byrd.
- Is Saliva a Route for COVID-19 Transmission? Salivary viral burden correlated with COVID-19 symptoms. They found matched nasopharyngeal and saliva samples displayed the same viral shedding dynamics. This data showed that the oral cavity is an important site for COVID-19 infection and implicated saliva as a potential route of COVID-19 transmission.
Another excellent article was published in the Journal of Pathology, “Salivary Glands Are a Target for SARS-CoV-2: A Source for Saliva Contamination,” Bruno Fernanades Matuck et al:University of São Paulo Medical School, July 7, 2021, Volume 254, Issue 3, SARS-CoV-2 Infects and Replicates in Salivary Glands. This article had an excellent electron microscope image showing coronavirus inside salivary glands: SARS-CoV-2 infects and replicates in the salivary glands.
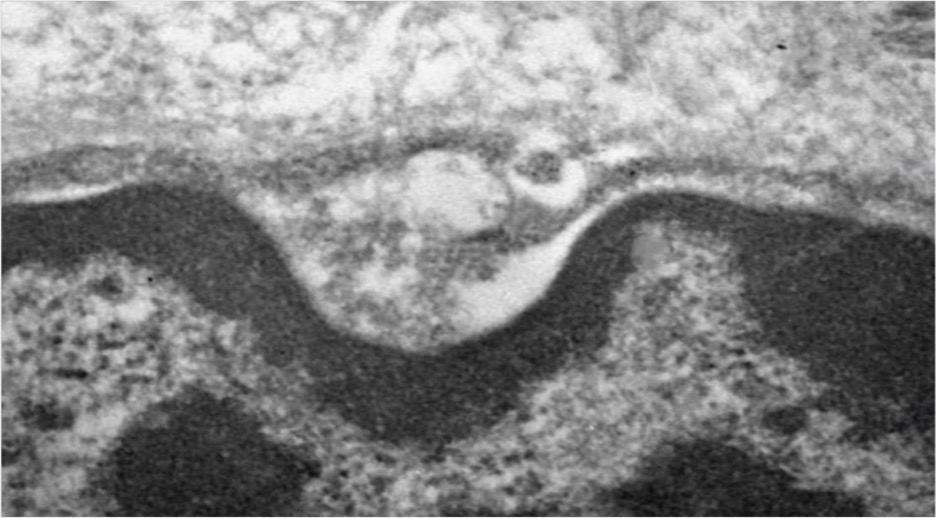
They went on to explain that, “Cells from salivary glands from patients who died from COVID-19 showed that tissues specializing in producing and secreting saliva served as reservoirs for the virus. This is why the virus is so abundant in saliva “This is the first report of a respiratory virus’s capacity to infect and replicate in salivary glands.”
They then asked the following question, “Why SARS-CoV-2 is so infectious?” They demonstrated the presence of RNA from SARS-CoV-2 in the periodontal tissue of patients who died from COVID-19. They then concluded that the virus may replicate in salivary gland cells and be present in saliva without coming into contact with nasal and lung secretions. Their next question was, Is the Virus Present in Tissue of Salivary Glands? So they autopsied 24 patients who died of COVID-19 then extracted tissue samples from the parotid, submandibular, and minor salivary glands. They found the virus was present in more than two-thirds of the samples. Their next question was, Can the mouth can be a direct point of entry for SARS-CoV-2? They found ACE2 and TMPRSS2 (these are the two needed entry level proteins) in various parts of the oral cavity, gum tissue and oral mucosa. Therefore: “The mouth could be a viable medium for the virus to enter the body directly.” They then asked, “What About the Saliva of Older People?” They found a high viral load even in older patients, who have less salivary tissue. “These patients had almost no salivary tissue, virtually no live gland cells, only fatty tissue. Even so, viral load was relatively high.”
They found patients with high levels of interleukin (IL-6), produced by periodontitis, were at significantly greater risk of suffering life-threatening respiratory problems. IL-6 is a plasma pro-inflammatory factor. Patients who have periodontitis before contracting COVID-19 are far more likely to die of respiratory failure. An analysis of the 153,000 (remember that this article was published in October of 2020) Americans who have died since the first COVID-19 cases were reported showed, “Gum disease has played and continues to play a role in the pandemic’s rising death toll.” They found that, “Periodontal Disease Generates IL-6.” Periodontitis increases IL-6 locally and systemically. Patients with bad gums face a much greater risk of generating IL-6 proteins that spread into their lungs and trigger a life-threatening respiratory crisis.” “Gum disease has been linked to other breathing ailments, including pneumonia and COPD”.

Hospitalized COVID-19 patients with periodontitis IL-6 levels above 80 pg./ml are 22 times more likely to suffer from acute respiratory problems and placed on a ventilator compared to patients with IL-6 levels below 80 pg/ml.
So when you feel like taking off your mask because you are hot or feel it’s difficult to breathe, or you decide not to get that next vaccine. When your patients don’t want to have that periodontal treatment you recommend, please just remember these articles. This way you will still be around and healthy when we have the next in-person ALD conference that we all can’t wait for. Stay vigilant, safe and healthy all of my friends.
Article written by Mel Burchman, DDS, MALD and ALD Past President
Email Dr. Burchman at [email protected]